



Challenging misconceptions about dental care.
There are widespread misconceptions about the importance of oral health that create challenges in advocating for dental reform.

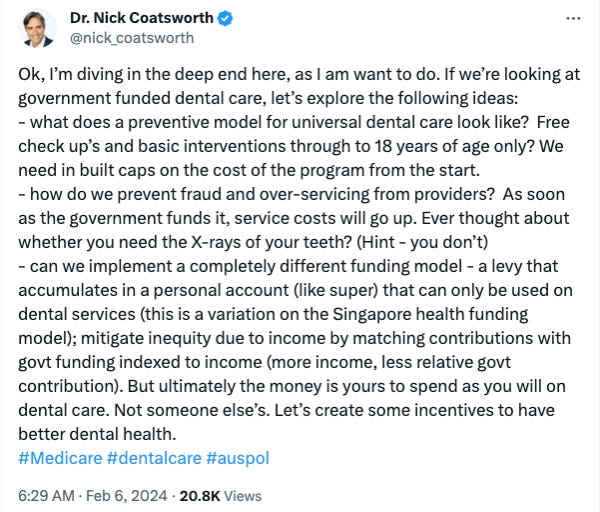
Earlier this week former deputy Chief Medical Officer of Australia Dr Nick Coatsworth weighed in on the issue of publicly funded dental care in a series of tweets, that in the process questioned the integrity and professionalism of dentists. Given that he has an influential platform in the national media and online, it’s worth looking at what was said and setting the record straight on a few misconceptions that he has put forth.

Coatsworth was responding to a tweet from a federal politician who was advocating to bring dentistry into Medicare – a long held policy position of the Greens. In doing so, he made a number of serious claims:
dentists would over-service if they had access to government funding
dentists would engage in fraud if they had access to government funding
government funding will inevitably lead to increased service costs
any publicly funded dental scheme needs to have caps or limits on spending
dental radiographs are not necessary.
Why does Coatsworth believe that dental practitioners in particular would engage in fraud and overservice if they had access to government funding? I looked the issue of overservicing in dentistry a few weeks ago, and there is no doubt that have been cases of fraud and misuse of publicly funded schemes such as the Medicare Chronic Disease Dental Scheme, but these issues do not appear to be widespread in dentistry. But medical practitioners have had access to government funding schemes for 40 years, so let’s look at the latest Medicare Professional Services Review report for January 2024, which identified a number of health practitioners who acknowledged having engaged in inappropriate practices in relation to a range of Medicare items:
a vascular surgeon acknowledged agreed to repay $310,000
a general medical practitioner agreed to repay $190,000
a general medical practitioner agreed to repay $290,000
a general medical practitioner agreed to repay $235,000
a general medical practitioner agreed to repay $295,000
There were no findings against any dental practitioners in January, but there was a case in December where a dental practitioner acknowledged having engaged in inappropriate practice in connection with rendering CDBS items 88161 and 88162 and agreed to repay $260,000.
Over-servicing and fraud appear to be an issue across all health professions, and it is not limited to dental practitioners, but it is a very small proportion of practitioners misusing these publicly funded schemes. Is that a reason to deny expanding public funding for dental services? And despite the claims, there does not appear to be any evidence that dental practitioners are more likely to engage in over-servicing or fraud than medical practitioners.
Will increased government funding of dental services increase the cost of those services? Perhaps Coatsworth is unaware that the government already funds some dental services through the Child Dental Benefits Schedule – around $300 million per year (admittedly a small amount in the context of overall dental expenditure). The CDBS has one of the highest bulk-billing rates across all of Medicare – at a time when bulk-billing rates for medical GP visits are dropping. There is no evidence that dental fees have increased in response to this government funding, Perhaps it could be argued that it hasn’t had an inflationary impact on dental fees because it forms a relatively small proportion of the overall treatment provided in the private sector, and that might change if bigger schemes were implemented. On the other hand private health insurance rebates contribute $2.2 billion dollars to dental care, yet dental fees have not increased at a rate greater than weekly earnings over the past 20 years.
The idea that dental practitioners would over-service or commit fraud, and that publicly funded schemes would increase service costs leads policy makers to the conclusion that dental schemes need to have caps or limits to them. This has been evident since the Chronic Disease Dental Scheme was introduced in 2004 (initially capped at $220 for the pre-cursor Enhanced Primary Care Dental Scheme, then increased to $2000 per year and subsequently $4250 over 2 years). The Teen Dental Scheme provided $150 vouchers and the Child Dental Benefits Scheme has a cap of $1095 over two years.
Just over 50% of children spend less than $400 of their CDBS cap, with only 12% spending more than $900. The problem with a cap, as the Fifth Review of the Dental Benefits Act 2008 found, is that it imposes an arbitrary limit which is insufficient to allow for necessary care for a small proportion of high-risk patients with complex or extensive treatment needs. This is why they recommended doubling the benefit cap for children considered ‘high care needs’ to ensure they receive adequate oral health care. The universal principles inherent in Medicare for the services that Coatsworth and his colleagues provide are not extended to publicly funded dental schemes, suggesting that dental health is somehow less important than the rest of health. This is an important misconception that needs to be corrected.
Finally, Coatsworth claims that dental radiographs are not necessary. This is an extremely ill-informed and misguided comment, that demonstrates how little other health professions understand dentistry. There is no nuance in this statement – perhaps we could have debated whether bitewing radiographs every 1 or 2 years are clinically indicated for all patients, or whether a risk-based approach should be taken, with a shorter duration for high-risk patients and a longer duration for low risk patients. This was a blanket statement that patients DON’T need radiographs.
One of my first major pieces of research many years ago was a comparison of radiographic and clinical diagnosis of approximal and occlusal dental caries in a young adult population. It clearly showed the importance of taking radiographs for caries diagnosis as part of a comprehensive dental examination. We found that, depending on the tooth surface, only 22.9-32.9% to 75.9-82.9% of tooth decay was able to be detected by clinical examination only. If patients took this advice to ignore having dental radiographs, then a large proportion of tooth decay would remain undetected until it had progressed much further – perhaps to the extent of causing pain and requiring root canal treatment or extraction – rather than being detected at an earlier stage where it could be treated more conservatively.
Perhaps the one area where we can agree is that there is a need to design a funding model that helps to increase access to dental care for those who are currently struggling, that has a strong focus on prevention and that has incentives to improve oral health.
In case you missed it ..
Episode 2 of the Dental As Anything podcast featuring Dr Jodie Heap talking about ethics and professionalism. You can find the episode here, or listen on Spotify or Apple Podcasts.